- Therapeutic Cataract & Refractive
- Lens Technology
- Glasses
- Ptosis
- AMD
- COVID-19
- DME
- Ocular Surface Disease
- Optic Relief
- Geographic Atrophy
- Cornea
- Conjunctivitis
- LASIK
- Myopia
- Presbyopia
- Allergy
- Nutrition
- Pediatrics
- Retina
- Cataract
- Contact Lenses
- Lid and Lash
- Dry Eye
- Glaucoma
- Refractive Surgery
- Comanagement
- Blepharitis
- OCT
- Patient Care
- Diabetic Eye Disease
- Technology
Fit pediatric cones with impression-based prosthetic scleral lenses













As many specialty contact lens fitters know, it’s not uncommon for a new patient to present with a handful of specialty contact lenses that didn’t work out as they had hoped. This scenario is all the more discouraging when contact lens practitioners give it their best shot yet fall short of success.
Even the most astute specialty lens practitioners have experienced this-myself included. Usually, I can brush off the disappointments, knowing that the next tough case will likely work out better than the one before. But when it comes to kids, it is a lot harder to say, “I’m sorry, but it’s never going to get any better.”
Meet Brayden
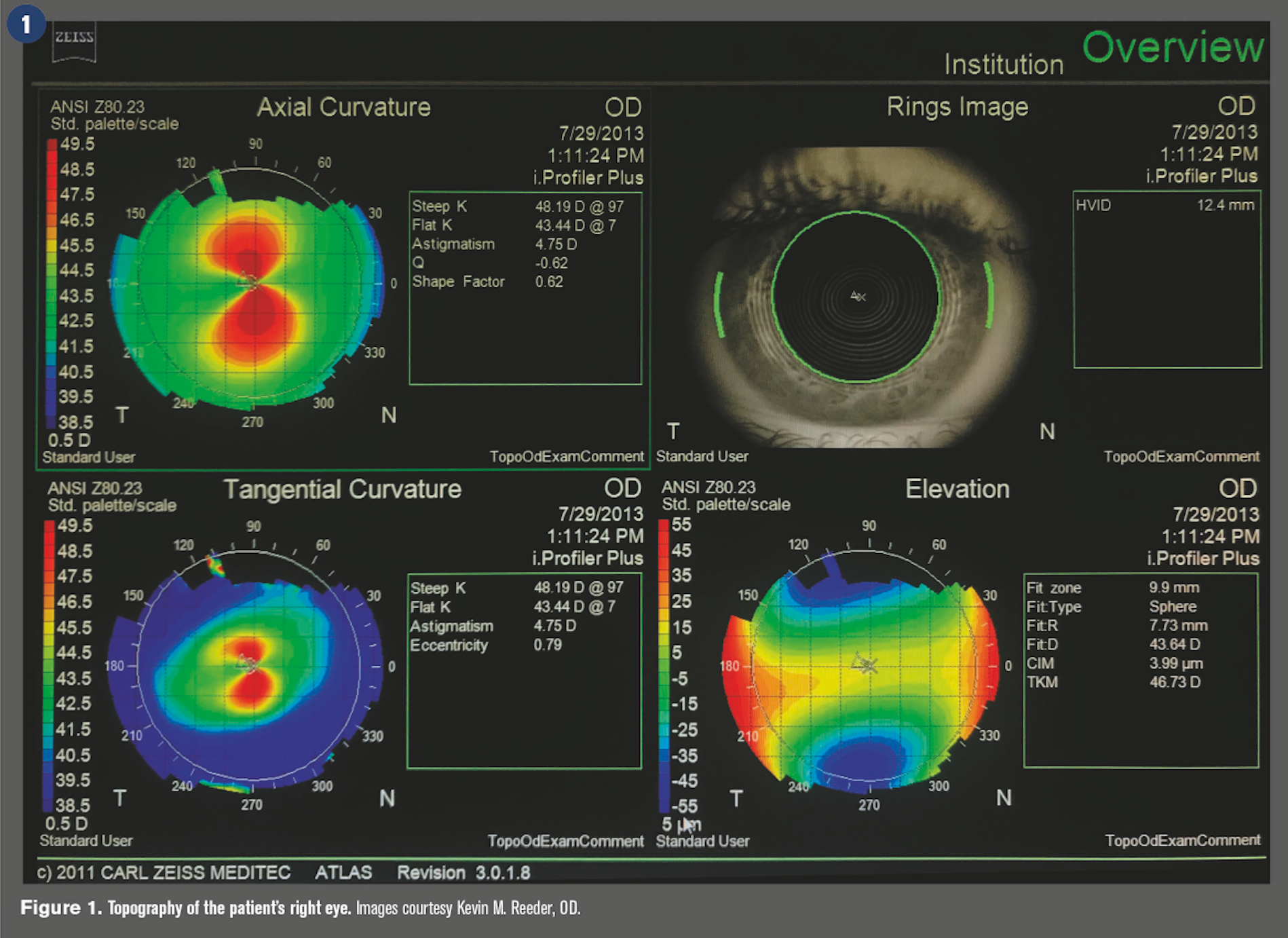
I was determined to find a way to help 11-year-old Brayden, whose family traveled down the California coast to help their little boy regain his vision. Brayden was diagnosed with keratoconus two years prior, but recently the condition began to progress rapidly. The decline was so swift and severe that by the time he saw the local ophthalmologist for a corneal evaluation, his visual acuity (VA) had dropped to 20/200.
Brayden was promptly treated with corneal cross-linking in both eyes to stabilize the keratoconus, but his vision remained distorted. Several gas permeable (GP) contact lenses were tried, but all failed to adequately correct the vision-particularly in his right eye.
Related: 7 strategies for fitting keratoconus patients
Lenses for keratoconus
Contact lenses are the primary means of vision correction for patients with keratoconus.1 Although soft lenses are often regarded as most comfortable and easiest for kids to apply, they are limited in masking irregular astigmatism2 and therefore typically are not an option unless the patient has forme fruste or early-stage keratoconus.3 For that reason, GPs are usually preferred.
Today, many GP lenses can provide excellent vision and relative comfort for patients with keratoconus. And, although these lenses require a learning curve, kids can-and do-learn application and removal quickly.
Related: Gas permeable contact lenses: special or not?
Modern GPs also come in an array of parameters, offering clinicians the benefit of flexibility. It was not that long ago that corneal lenses were the most common form of rigid lens used for keratoconus.4 Today, however, we recognize the advantages of larger-diameter contact lenses in terms of decreased lens awareness and onâeye stability, and we are therefore seeing a surge in corneo-scleral, mini-scleral, and scleral lens fitting for keratoconus.5
By the time Brayden arrived in my practice, he had already tried a few different lenses with experienced practitioners, and I too tried my hand at creating a suitable scleral lens design. In fact, I tried five different scleral designs, but all were uncomfortable and the patient could wear them for only one to two hours.
The greatest challenge was in the right eye. Braydon was comfortably wearing a soft lens OS, but the disparity was enormous. He couldn’t function and was growing frustrated.
Paradigm shift needed
Despite the outstanding advances in lens technology, patients like Brayden continue to present with problems we can’t solve. As Downie and Lindsay pointed out in their comprehensive review, there is a need for an individualized approach to contact lens fitting for patients with keratoconus.6 I couldn’t agree more, which made me very thankful when I found just that-an individualized lens option that was stunningly easy to fit.
I was offered the opportunity to receive specialized training and certification for a relatively new scleral lens that is fit using an impression technique. The lens, called EyePrintPRO, is similar to a standard scleral in that it is made of the same FDA-approved oxygen permeable materials and the fit vaults the cornea while landing on the sclera. However, this lens is fit in a different way. Instead of using a series of curves, EyePrintPRO is designed using Elevation Specific Technology to exactly match the unique irregularities of each individual eye.
EyePrintPRO is like a fingerprint-it’s completely individual. The process begins with an EyePrintPRO impression using a polyvinyl siloxane material. Doctors then send the impression to an EyePrintPRO lab for 3-D scanning. The scanned data is used to produce a lens that matches the impression exactly and therefore fits perfectly. This is what makes EyePrintPRO so very different compared to previous options-it is a completely custom scleral lens that matches the exact contours of the anterior surface of the globe. The lenses are treated with Tangible Hydra-PEG (Tangible Science) to improve surface wettability, increase lubricity, and reduce protein and lipid deposition.
I wondered if an EyePrintPRO lens could be the answer for Brayden-and so many others like him. I agreed to the training and was excited to see what I could do with this new lens.
Convincing his mother
Upon learning about EyePrintPRO, my enthusiasm was greater than that of the patient’s mother. In fact, at that time she was on the verge of giving up and considered seeking care elsewhere.
I explained that the technology, although new at the time, was proving to be successful in patients with keratoconus. If that didn’t convince her, I explained that a company representative was coming to the office to train me-and Brayden could be fit that same day.
Because the company requires that doctors learn the impression technique, an experienced EyePrintPRO fitter comes to practices to certify fitters. To offset the cost of this training, the company discounts the cost of lenses fit that day. In fact, the company encourages fitters to schedule their toughest cases so the trainer can help fitters with them during the training.
This method works well for EyePrintPRO fitters because, according to the company, ordering records reveal first-lens success 67.3 percent of the time. If revisions are needed, 75 percent are due to a lens power change only. Company representatives say fitters achieve about a 95 percent success rate within two lenses.
Happy endings
Brayden’s EyePrintPRO lens arrived about 10 days after the fitting, and he said it was the most comfortable lens he had ever worn-including three soft lenses, five scleral lenses, and one hybrid lens. Not only did Brayden experience virtually no lens awareness, he could see very well.
Moments after he applied the lens, he was one line away from 20/20 VA OD. And the improved vision in his right eye allows him to wear a lower power lens OS.
Plus, Brayden experienced binocular vision, and it has changed his life. Today, his best-corrected visual acuity OU is 20/20, and he is able to play baseball. Brayden’s mother is very happy as well.
What I learned during Brayden’s EyePrintPRO fitting process changed the way I approach tough contact lens fits, especially in pediatric patients.
Related: How to successfully perform a pediatric eye exam
Pediatric optometry is challenging, especially in patients with corneal disease. Primary eyecare providers must recognize that these children have their whole lives ahead of them, and providers can effect big change in their lives by fitting them with new contact lens technology or referring to another eyecare provider who can. As I experienced firsthand with Brayden, even after a string of failures, eyecare providers can be the heroes that these kids need.
References:
1. Bilgin LK, Yilmaz S, Araz B, Yuksel SB, Sezen T. 30 years of contact lens prescribing for keratoconic patients in Turkey. Cont Lens Anterior Eye. 2009 Feb;32(1):16-21.
2. Griffiths M, Zahner K, Collins M, Carney L. Masking of irregular corneal topography with contact lenses. CLAO J. 1998 Apr;24(2):76-81.
3. Jinabhai A, Radhakrishnan H, Tromans C, O'Donnell C. Visual performance and optical quality with soft lenses in keratoconus patients. Ophthalmic Physiol Opt. 2012 Mar;32(2):100-16.
4. Morgan PB, Woods CA, Tranoudis IG, Efron N, Knajian R, Grupcheva CN, et al. International contact lens prescribing in 2008. CL Spectrum. 2009;24(2):28-32
5. van der Worp E. A guide to scleral lens fitting. Available at: https://commons.pacificu.edu/mono/10/. Accessed 8/17/18.
6. Downie LE, Lindsay RG. Contact lens management of keratoconus. Clin Exp Optom. 2015 Jul;98(4):299-311.
7. van der Worp E, Bornman D, Ferreira DL, Faria-Ribeiro M, Garcia-Porta N, González-Meijome JM. Modern scleral contact lenses: A review. Cont Lens Anterior Eye. 2014 Aug;37(4):240-50.
8. Nguyen MTB, Thakrar V, Chan CC. EyePrintPRO therapeutic scleral contact lens: indications and outcomes. Can J Ophthalmol. 2018 Feb;53(1):66-70.