- Therapeutic Cataract & Refractive
- Lens Technology
- Glasses
- Ptosis
- Comprehensive Eye Exams
- AMD
- COVID-19
- DME
- Ocular Surface Disease
- Optic Relief
- Geographic Atrophy
- Cornea
- Conjunctivitis
- LASIK
- Myopia
- Presbyopia
- Allergy
- Nutrition
- Pediatrics
- Retina
- Cataract
- Contact Lenses
- Lid and Lash
- Dry Eye
- Glaucoma
- Refractive Surgery
- Comanagement
- Blepharitis
- OCT
- Patient Care
- Diabetic Eye Disease
- Technology
Pearls on diagnosing and managing glaucoma for optometrists

Optometrists can play an important role in early detection, earlier surgical referral to experienced skillful surgeons, surveillance, and follow-up care for glaucoma patients.
Optometrists play an important role in the detection and management of glaucoma.
In healthy eyes, the mean intraocular pressure (IOP) is 15 mm Hg, while the mean IOP in patients with untreated glaucoma is 18 mm Hg.1 The age-related enlargement of the lens is the most identifiable cause of glaucoma.2


Laroche


Rickford
Thus, individuals with an IOP of 18 mm Hg or higher should be evaluated using gonioscopy to look for either angle closure or increased pigment deposition inferiorly that may contribute to the increased IOP. These two findings are the most common causes of glaucoma seen in my practice (DL).
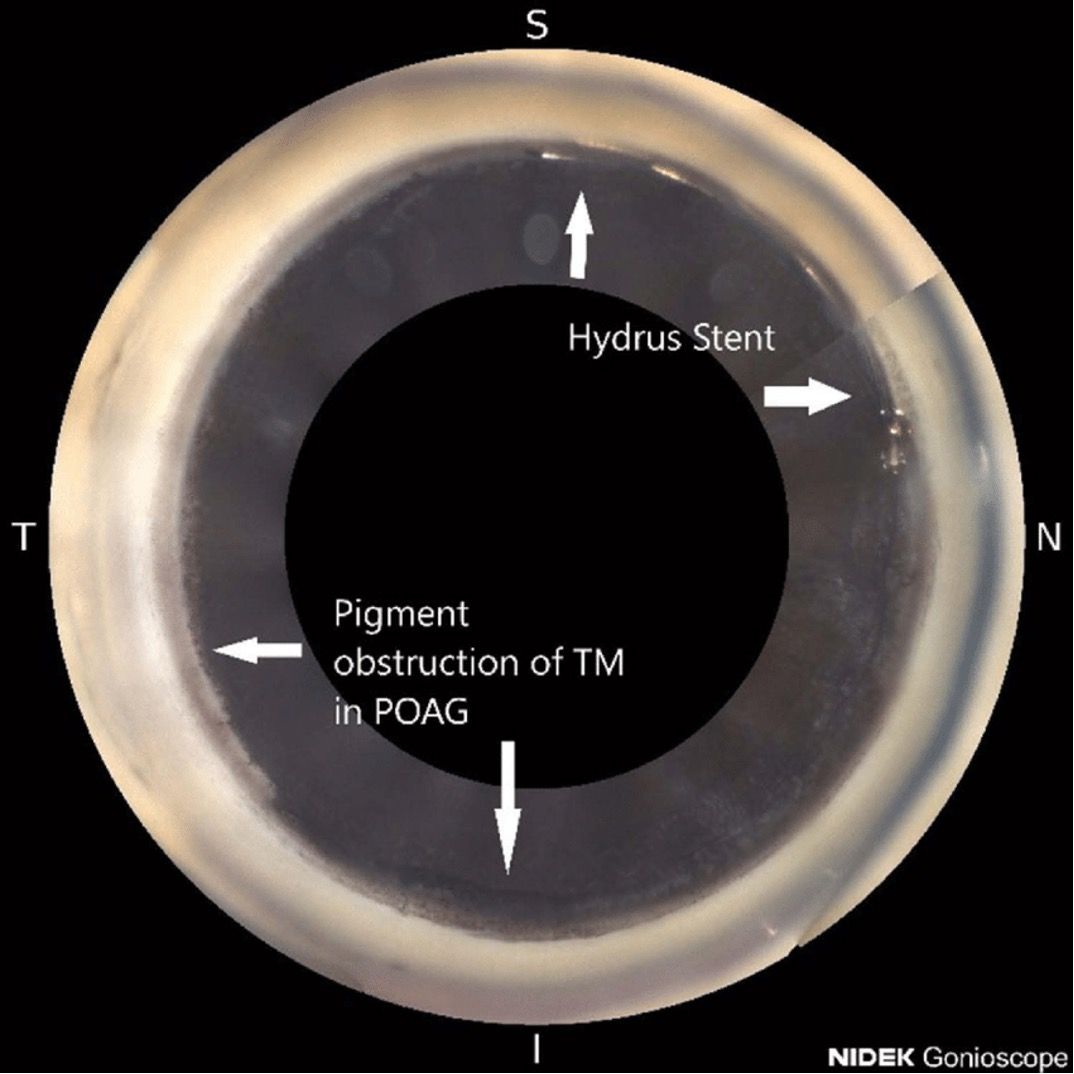
Figure 1 (below) shows greater pigment obstruction of the trabecular meshwork (TM) inferiorly than superiorly with a Hydrus stent (Ivantis, Inc). The stent scaffolds Schlemm’s canal, bypassing the TM in a deeper anterior chamber after cataract surgery.
Diagnosing glaucoma
The loss of retinal ganglion cells and axons within the optic nerve of glaucomatous eyes results in the characteristic optic nerve cupping.3
In assessing for glaucoma, the optic nerve should be carefully assessed for cupping, and the cup-to-disc ratio should be evaluated and documented.
Optic nerve head photos, visual field tests, and a baseline optical coherence tomography (OCT) imaging should also be obtained to detect abnormal nerve fiber layers.

 with a Hydrus stent, image with NIDEK Gonioscope")
Figure 1. Pigment obstruction of the trabecular meshwork (TM) with a Hydrus stent, image with NIDEK Gonioscope.
Additionally, central corneal thickness (CCT) should be measured. The normal CCT is about 545 μm.4
Prior studies examining the correlation between CCT and IOP have demonstrated thicker corneas yielding higher IOP readings and thinner corneas yielding lower IOP readings.5,6
Measuring CCT in patients with glaucoma may help identify those with thinner corneas who are at higher risk for progression and will require lower IOP targets.
Management of glaucoma
If a patient is diagnosed with glaucoma, current treatment options include topical medications to lower IOP and/or selective laser trabeculoplasty (SLT).
Although these therapies are successful in slowing the pace of glaucoma progression, it is often not enough to fully prevent glaucoma from advancing and sufficiently lowering IOP to target levels.
Many patients have compliance issues with medical therapy and diurnal IOP fluctuation. Cataract surgery has been utilized as an effective glaucoma treatment through its ability to reduce IOP particularly in angle-closure glaucoma patients.7-9
Early cataract surgery and MIGS
Recent improvements in cataract surgery technology have made it much safer today than 20 years ago. Novel surgical treatment options and devices have been developed to treat glaucoma.
Of these, microinvasive glaucoma surgery (MIGS) has gained more interest and popularity. MIGS uses stents, microcatheters, and surgical techniques to further lower IOP at the time of cataract surgery and aims to cause as little trauma to the eye as possible.10
MIGS can be used as an adjunct to cataract surgery and improve the patients’ quality of life (QOL) by maintaining long-term control of IOP, slowing glaucoma progressions, and decreasing dependence on daily topical eye medications.11-14
In my practice (DL), I have transitioned to offer early cataract surgery/clear lensectomy with an intraocular lens and microinvasive glaucoma surgery in patients over 50.2 The earlier these procedures are performed, the greater success rate you can have.
In comparison to laser peripheral iridotomy, clear lens extraction is associated with better clinical and QOL outcomes in patients with early or moderate primary angle-closure glaucoma (PACG) and patients with an IOP over 30 mmHg.15

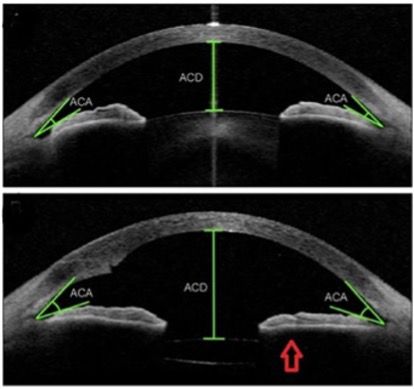
, preventing iridolenticular contact and eliminating the release of pigment from obstructing the trabecular meshwork.")
Figure 2. Anterior segment OCT demonstrating how lens extraction opens the anterior-chamber angle (ACA), preventing iridolenticular contact and eliminating the release of pigment from obstructing the trabecular meshwork.
Often following early surgical intervention with cataract surgery and MIGS, patients have a sustained reduction in glaucoma medications.16 Further, the number of additional glaucoma surgeries needed following trabeculectomy or glaucoma tube-shunt surgery is dramatically decreased.16
These lower IOP through a process of removing the enlarged lens from the eye, expanding Schlemm’s canal, and bypassing the obstructed trabecular meshwork to restore outflow to the distal collector channels.
This procedure can also be performed in an affordable manner using an ophthalmic MVR blade and Sinskey hook in resource poor areas. This is especially important in vulnerable, poorer population groups with less access to medications and follow-up care.
A recent study by Okuda et al. showed a significant association between surgical failure and glaucoma patients with a history of a long duration of anti-glaucoma medications that had undergone MIGS.17
Using propensity score matching analysis, the study showed that patients with a history of less than 4.5 years of anti-glaucoma medication usage had significantly higher success rates than the greater than 4.5-year users (72% versus 52%; p = 0.04).17

")
Figure 3: Affordable goniotomy bypassing pigment obstruction of the trabecular meshwork performed with less expensive MVR blade and Sinskey hook. (All images courtesy of Daniel Laroche, MD, and Kara Rickford, MS.)
To ensure a successful outcome, optometrist should locate an experienced cataract and glaucoma surgeon proficient in early cataract surgery and MIGS.
It is important to have experienced surgeons that can achieve successful outcomes and be able to avoid and manage complications of cataract surgery.
Such complications are rarer these days in experienced skillful surgeons, but do include infection, hyphema, uveitis, retinal detachment, lens fragments, fluid buildup in the retina, ptosis, light sensitivity, hemorrhaging, floaters, dislocated intraocular lens, or postoperative rise in IOP.18
Medical therapy
After successful cataract surgery and MIGS, many patients will not need medications and will often have less diurnal IOP variation.
The HORIZON trial compared combined cataract surgery and microstent with cataract surgery alone and found that 66% of the eyes treated with the microstent were medication free at the 5-year follow-up compared to 46% in the cataract surgery group (P<0.001).19
The combined surgery group also included a higher proportion of eyes with an IOP of 18 mm Hg or less and a greater likelihood of IOP reduction.19
Laser surgery
SLT after cataract surgery has been shown to be effective when needed in reducing IOP and postoperative medication dependency. The IOP-lowering effect of SLT is comparable between phakic and pseudophakic eyes.20
SLT surgery following combined MIGS, cataract extraction, and iStent implantation has been shown to be successful in terms of glaucoma medication reduction in iStent patients.21
Over the years, glaucoma detection, treatment, and management have seen several shifts that have improved surgical procedures and patient outcomes.
The future of glaucoma care is here and now, and optometrists can play an important role in early detection, earlier surgical referral to experienced skillful surgeons, surveillance, and follow-up care.
Some rare secondary glaucoma such as neovascular, uveitis, congenital, and others may not be suitable for earlier cataract surgery and MIGS. Glaucoma continues to require and individualized approach.
About the authors
Daniel Laroche, MD, is president of Advanced Eyecare of New York and clinical associate professor of ophthalmology at New York Eye and Ear of Mount Sinai Icahn School of Medicine, in New York City, New York.
Kara Rickford, MS, is a medical student at New York Medical College in Valhalla, New York.
---