
Telemedicine in the face of COVID-19
An eyecare group in a New York City hospital shares its protocol.







When the American Optometric Association advised optometrists to postpone all routine eye care visits on March 19, 2020, many ODs turned to telehealth. Virtual visits have many advantages, like keeping patients safe from coronavirus exposure, improved access to care, and reduced health care costs. It is essential to have a written plan when incorportating telemedicine, before implementation.
Plato may have said that necessity is the mother of invention but now that COVID-19 has demonized the world, Plato’s words have taken on an international urgency. It has manifested in the rapid innovations we are witnessing, including complex adaptations used to split ventilators between patients, rapid development of antiviral medications and vaccines, expedited clinical trials, the temporary relaxation of regulatory rules, and the redeployment of medical personnel to perform duties outside of their normal scope of practice. The magnitude of the response is matched to the magnitude of the necessity.
Amid this surge of ingenuity, telemedicine has been born in the epicenter of this crisis at the Department of Ophthalmology at Columbia University Medical Center in New York City. We share with you pearls that we have learned which highlight the importance of timely implementation of telemedicine into practice and suggestions for a triage system with a step-wise approach to encourage success.
Related: Dr. Ernie Bowling discusses dry eye in the digital age
Telemedicine in eye care was until now more of a concept than a fully developed reality, a topic of interest that was discussed at professional meetings for many years, a possible wave of the future. In the midst of the COVID-19 pandemic, telemedicine is no longer a futuristic concept.
Telemedicine is our new reality. And it has become a reality overnight fraught with new levels of connection between physicians and patients, legal responsibilities in obtaining consent and submitting proper documentation, and lastly, learning new billing languages of the virtual world.
Although seemingly daunting, spending time on a plan of action that takes into account known hurdles prior to implementation can make the difference between a successful and failed attempt. And in this situation, one in which our patients need our help, our staff needs protection, and our offices need to stay afloat, failure is not an option.
Related: Dry eye in the digital age
Our approach to telemedicine
A strong telemedicine initiative was started in our department during the first week of March as a way to continue delivering care while simultaneously implementing practices that prevented the spread of the COVID-19 virus.
By the first week of April it had become the dominant form of patient contact in our department.
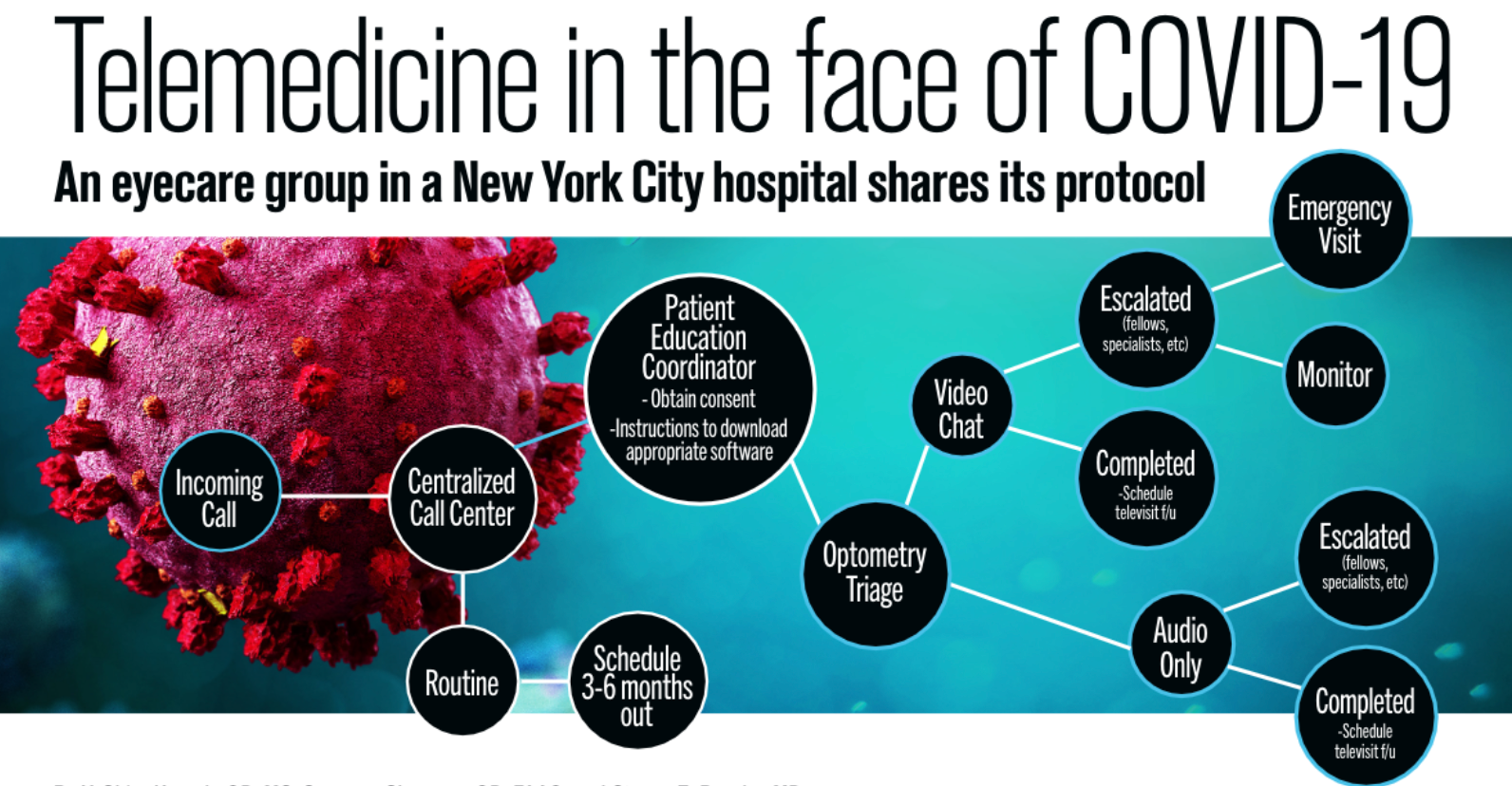
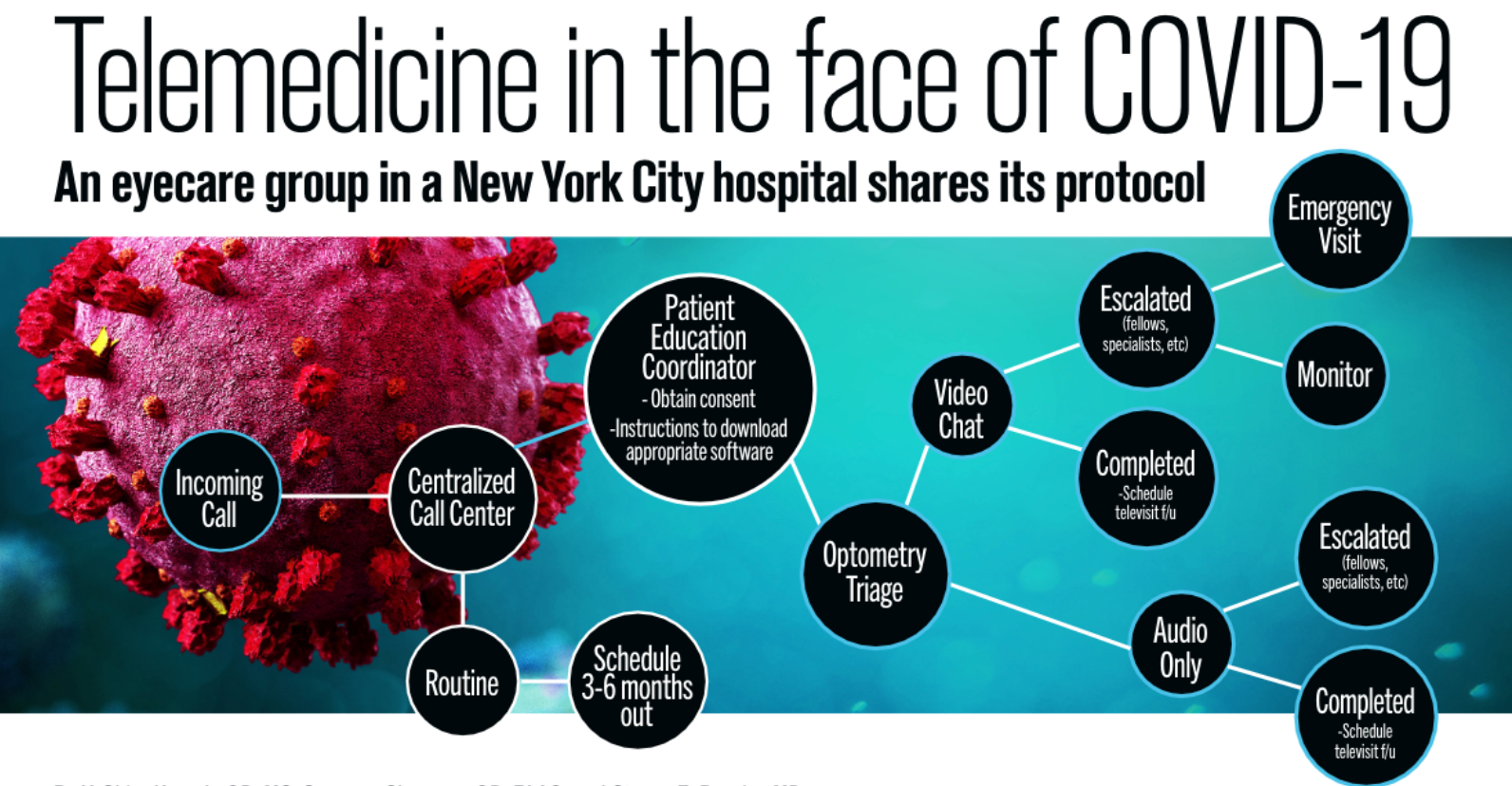
Our telemedicine example was initially geared to allow for an effective triage system for new and established patients and involved the collaboration of scheduling personnel, technicians, practice administrators, optometrists, and ophthalmologists.
Related: 10 new treatments in eye care
With the luxury of an electronic medical records (EMR) system with a built-in Health Insurance Portability and Accountability Act (HIPAA)-compliant platform to enable immediate use, providers completed required on-boarding and immediately began scheduling visits.
The temporary relaxation of privacy requirements from national leadership allowed us to use audiovisual communication platforms, including FaceTime, Skype, Google Hangout, and others that would not normally be approved for patient visits. These policies-needed to cope with the emergency conditions we confronted-improved our ability to extend care to patients with varying levels of “tech-saviness.”
Further developments included the use of com-mercially available apps such as.... for patients to measure their own visual acuity, color vision, and the Amsler grid. Improvised techniques were developed to check for afferent pupil defects, confrontation visual fields, defects in extraocular movement, and strabismus.
These approaches enabled us to implement effective triage and recommend basic management. Patients with vision-related concerns that were deemed to be urgent or were inadequately evaluable by these means were scheduled for in-person visits.
Related: Chris Wroten, OD: New technologies and pharmacology
Triage pearls
Over the past month, we have learned a considerable amount about the process and what our current state of telemedicine can offer. When deciding to bring telemedicine into your practice there are a few pearls to take into consideration. To start, the primary focus should be an effective triage system. See Figure 1.
The time is now
– Get organized with a designated team
– Create a telemedicine triage protocol
– Delegate specific tasks
– Develop office protocols for key operations, including scheduling, patient instruction, allotted times for televisits, and billing
– Schedule regular meetings to review the process. Iron out kinks at the end of each day for the first week, then every other day, and move toward having a weekly meeting
Related: How I have been using telemedicine amid COVID-19
Decide on a platform to perform televisits
– Some EMR systems have HIPAA-compliant software that can be used for this purpose. If not, additional software may have to be purchased. Although regulations surrounding HIPAA have been relaxed during the COVID-19 state of emergency, it is best to have appro-priately compliant software to future-proof telemedicine needs and train staff from the beginning. Even in the current environment, patient privacy still matters
Related: Video: Why I wear scrubs in the office during COVID-19
Patient consent is necessary
– Patients must be informed that the session will constitute an actual examination and be billed as such. Consult with liability carrier for the specific language and format recommended
Related: Fashion advice from an OD on the frontlines of COVID-19
Understand the limitations
– Current technologies will not allow detailed examination of the anterior or posterior seg-ment of the eye
– It is not possible to measure intraocular pres-sure (IOP)
– Patient-reported measures, like visual acuity, may not be highly reliable
– Refraction is not possible
– Some patients are more tech-savvy than others
– Patients with low vision will need special assistance on their end
– Some patients will need to be seen in the office, and these patients and visits should not be overlooked. Stand-alone televisits are inappropriate for these patients and should be handled as such
Related: NASA awards $5 million to artificial retina development efforts
Learn the billing codes
– The billing compliance requirements, at least for now, are different than those needed for in-person examination
– Review codes with billing team
Perform internal auditing
– Conduct an audit at least after the first week of televsit piloting and learn how to improve. Best practice is to audits for the entire first month of telehealth.
Related: Expert advice on safe contact lens wear during COVID-19
Get the most out of a televisit
Consider implementing these suggestions in order for both the doctor and the patient to gain as much as benefit as possible from a telehealth visit.
Instructions for patients prior to televisits should include:
– Necessary software downloaded with education from staff about usability and test for functionality
– Instruction to download additional helpful apps, if possible. This may include a visual acuity chart, Amsler grid, color vision plates, etc.
– Instruction for pertinent ocular and medical histories to be readily available to review with physician during the visit or to email prior to the visit
– Submission of photos through a secure platform
Related: 5 facts about contact lens wear with COVID-19
During the visit:
– Obtain and document verbal consent
– Patient should sit in well-lit room
– Patient should have family member or friend available for assistance during the visit, if appropriate
– Headphones recommended during visit with patient so the doctor’s hands are free to demonstrate various things to patients
Related: Hope in the time of COVID-19
After the visit:
– Document all that transpired immediately, including start and end times of the visit
– Include review notes, impression and plan, photo-documentation, interpretation and report, and billing codes
– Create list of all patients seen via televisits to review later with billing staff
– Schedule follow-up as necessary
Summary
Amid the COVID-19 pandemic, telemedicine has emerged as an essential technology for all healthcare professionals. In our experience, we have learned it is essential to have a written plan for how to incorporate telemedicine into daily practice prior to implementation.
Utilize resources such as the American Optometric Association (AOA), American Academy of Optometry (AAOptom), and American Academy of Ophthalmology (AAOphth) to aid in formulating documentation and triage protocols.
It is important to learn from each other’s experiences as ODs continue to expand the use of telemedicine in to deliver eye care, especially in times like this, when in-person visits are severely limited.
More by Dr. Kresch: The myopia epidemic: Are new therapies in sight?











Newsletter
Want more insights like this? Subscribe to Optometry Times and get clinical pearls and practice tips delivered straight to your inbox.












 of patients believe that medical technology innovations will enhance care for the aging population, with 90% of providers recognizing the need to address specific requirements for older patients. Image credit: AdobeStock/buritora")




