
Keratoconus overview: History, etiology, and diagnosis
Much has changed in the study of keratoconus over the years.


(Image credit: Adobe Stock / bigguns)

Keratoconus is a disease of the cornea that, if left untreated, can lead to loss of vision, decrease in quality of life, and potentially blindness. As optometrists, we are the gatekeepers of the management of keratoconus, barring the increasingly reduced amount of partial or full-thickness corneal surgical transplants performed. In the United States, this is because we now have an FDA-approved, safe, and effective incision-free treatment/procedure—corneal cross-linking (CXL)—to halt or slow the progression of this increasing public health concern.1
Outside the United States, CXL has long been a primary method to stop this disease in its tracks. Patients who present with keratoconus can expect to be patients in our practices for the vast majority of the continuum of the disease (in other words, for the rest of their lives). We diagnose, assess, and treat. We advise on best patient practices and prescribe simple to very advanced refractive tools for best corrected vision and best quality of life. We monitor for change and progression and adapt our treatment modality accordingly. The only reason why a patient would potentially leave for ophthalmologic care include CXL treatment; surgical management of hydrops via pneumatic descemetopexy (anterior chamber air or gas bubble to tamponade Descemet membrane) or removal of permanent corneal scarring; or corneal transplant.
History
Dr John Nottingham is widely cited as the first author to formally define keratoconus, after his Treatise on the Conical Cornea was published in 1854. As the first to consolidate and the varying symptoms, Nottingham was also the first to discuss the origins of customized contact lenses. These lenses, he said, were “lenses with posterior surface corresponding to the front of the eye, and anteriorly of regular figure, are amongst the means proposed for correcting the altered refraction; along with these may be mentioned lenses of transparent animal jelly, contained in capsules of glass, to be placed on the front of the eye.”2
However, for 150 years prior to this, it should be noted that other eye care providers and researchers discussed parts of the disease of keratoconus but not in its entirety.3 Nottingham gave credit to his predecessors, and it is noted that understanding of the disease, at least in part, dates back to the late 1600s and early 1700s.
As better understandings of ophthalmic and nonophthalmic diseases progressed, it was recognized in the research community that understanding the impact of a given disease in the public domain was important to overall awareness, allocation of resources, and individual clinical efforts. The establishment of data regarding prevalence and incidence of a given disease began to take on particular public importance. Prevalence (sometimes referred to as prevalence rate) is the proportion of persons in a population (new and existing) who have a particular disease or attribute at a specified point in time or over a specified period of time. Incidence refers to the occurrence of new cases of disease or injury in a population over a specified period of time.4 For example, if a clinician was aware that a particular disease had a prevalence in the population of 1:250, it will be suspected in a differential diagnosis list much more acutely during patient encounters than if the prevalence rate was 1:250,000. This is an important concept to understand as we look at how the prevalence and incidence of keratoconus has increased over the past 30 to 40 years.
Epidemiology of keratoconus
If you have done any amount of reading or research on keratoconus, you will commonly find the following epidemiological statements: The incidence has been reported to be approximately 1 in 2000, and the prevalence is estimated to be 54.5 per 100,000.5 At the time of publication, this may have been the most accurate data we had, but not today. The Kennedy et al study, A 48-Year Clinical and Epidemiologic study of Keratoconus, needs to be fully investigated and have the sheets pulled back for a detailed understanding of how these numbers came about. Here are some facts about the study and how these estimates were established:
- The study date range was from 1935-1982.
- The sample size was 64 individuals from 1 county in Minnesota.
- The age range was 12 to 77 years (only 4 were older than 40 years).
- The diagnosis of keratoconus was developed on the basis of characteristic irregular light reflexes the examiner observed during ophthalmoscopy or retinoscopy or irregular mires during keratometry
- The paper insinuates that all subjects were White, as the incidence rate was adjusted by age and sex to the White population of the United States.
Of particular note, there was no objective testing, no crossover clinician evaluation, no pachymetry recorded, no evaluation outside of the central 3 mm of the cornea, no evaluation outside of the visual axis, and, most importantly, there was no computerized topography or tomography of any kind. Although the Scheimpflug camera/tomographer is the device of choice today for evaluation of the keratoconic cornea, not even the workhorse of the industry, the corneal topographer, was utilized. Needless to say, this information is of high bias, low reliability, significant limitation, and of only historical value.
In addition (and a significant historical note), the corneal topographer itself was not necessarily commercially available until the early to mid-1990s. Therefore, diagnosis of keratoconus for the purposes of prevalence and incidence was not made by objective computerized evaluation of the cornea, yet we still cite these values today. This needs to change immediately. Clinicians must be aware of the most accurate prevalence and incidence estimates to guide their clinical practice appropriately and for the patient’s best interest.
So, what is the most accurate estimate on prevalence and incidence of keratoconus today? The answer is: It depends. Although we know the numbers are significantly higher than was previously reported, there is variance in worldwide population studies depending on a variety of factors, one of which being the variance of testing and reporting. If a study were to ever be developed that can look at a large population within 1 medical records system and use similar testing methods and equipment, a much more accurate estimation could be extrapolated. In 2016, Godefrooij et al published just that. In the Netherlands-based study, Age-Specific Incidence and Prevalence of Keratoconus, the Dutch database of 4.4 million individuals ages 10 to 40 years were evaluated for keratoconic disease. The shocking results were that values reported for keratoconus incidence and prevalence were 5- to 10-fold higher than previously reported for values in population studies.1
Ethnicity
Although gender does not seem to be a factor in keratoconus, ethnicity does play a role. Keratoconus prevalence has been shown to vary between ethnic groups. A paper by Gordon-Shaag et al stated that “it was first noted by Pearson et al who found that Asians [Indian, Bangladeshi, and Pakistani] living in the English Midlands had an incidence of the disease 4.4 times higher than in White [individuals].6 This was confirmed in 2 other investigations that were also conducted in the English Midlands, where the difference in incidence was 7.5/1 and 9.2/1.”7-9 Therefore, it is important to understand the demographics of the keratoconus suspect to assist in the diagnosis and risk opportunity.
Global consensus of corneal ectasias
Today, we have much more advanced equipment for early detection, a global definition of mandatory findings to diagnose the disease, the ability to monitor for progression, advanced medical and ophthalmic devices to improve visual acuity and quality of life, and treatment methods to halt the progression of the disease.
In a landmark Cornea paper from April 2015 titled Global Consensus on Keratoconus and Ectatic Diseases, representatives from the 4 major cornea societies around the globe convened to establish the definitions, concepts, clinical management, and surgical treatments. The group defined keratoconus as a progressive, bilateral, asymmetric progressive disease of the cornea with environmental and genetic etiologies, which is part of a family of diseases named corneal ectasias. The 4 diseases that make up the corneal ectasias include the following:
- Keratoconus
- Keratoglobus
- Pellucid marginal degeneration (PMD)
- Postrefractive surgical ectasia
According to Gomes et al, a consensus was achieved regarding the statements “keratoglobus and keratoconus are different clinical entities” and “true unilateral keratoconus does not exist.” In addition, the “thinning location and pattern are aspects that distinguish keratoconus, PMD, and keratoglobus.” The group considered central pachymetry to be “the least reliable indicator [or determinant] for diagnosing keratoconus, because keratoconus can be present in a cornea of normal central thickness.” These consensus statements regarding the disease itself led to the following statement regarding the devices required to evaluate the cornea for keratoconus. “There was consensus that tomography is currently the best and most widely available test to diagnose early keratoconus. Posterior corneal elevation abnormalities must be present to diagnose mild or subclinical keratoconus. Specifically, certain parts of the cornea need to be evaluated for earliest signs of disease.” Optometrists must be aware that tomographic Scheimpflug cameras that can evaluate the elevation of the posterior surface of the cornea for signs of ectasia must be implemented at this time for earliest identification of disease.
Mandatory findings to diagnose keratoconus
- Abnormal posterior ectasia
- Abnormal corneal thickness distribution (eg, as seen with abnormal corneal thickness spatial distribution)
- Clinical noninflammatory corneal thinning
The exact values for any parameter will vary based on the machine being used and, for elevation values, the reference surface. Additionally, the values will vary if one is screening (eg, refractive surgery) where sensitivity is the overriding concern or treating (eg, CXL) where specificity assumes greater significance.10


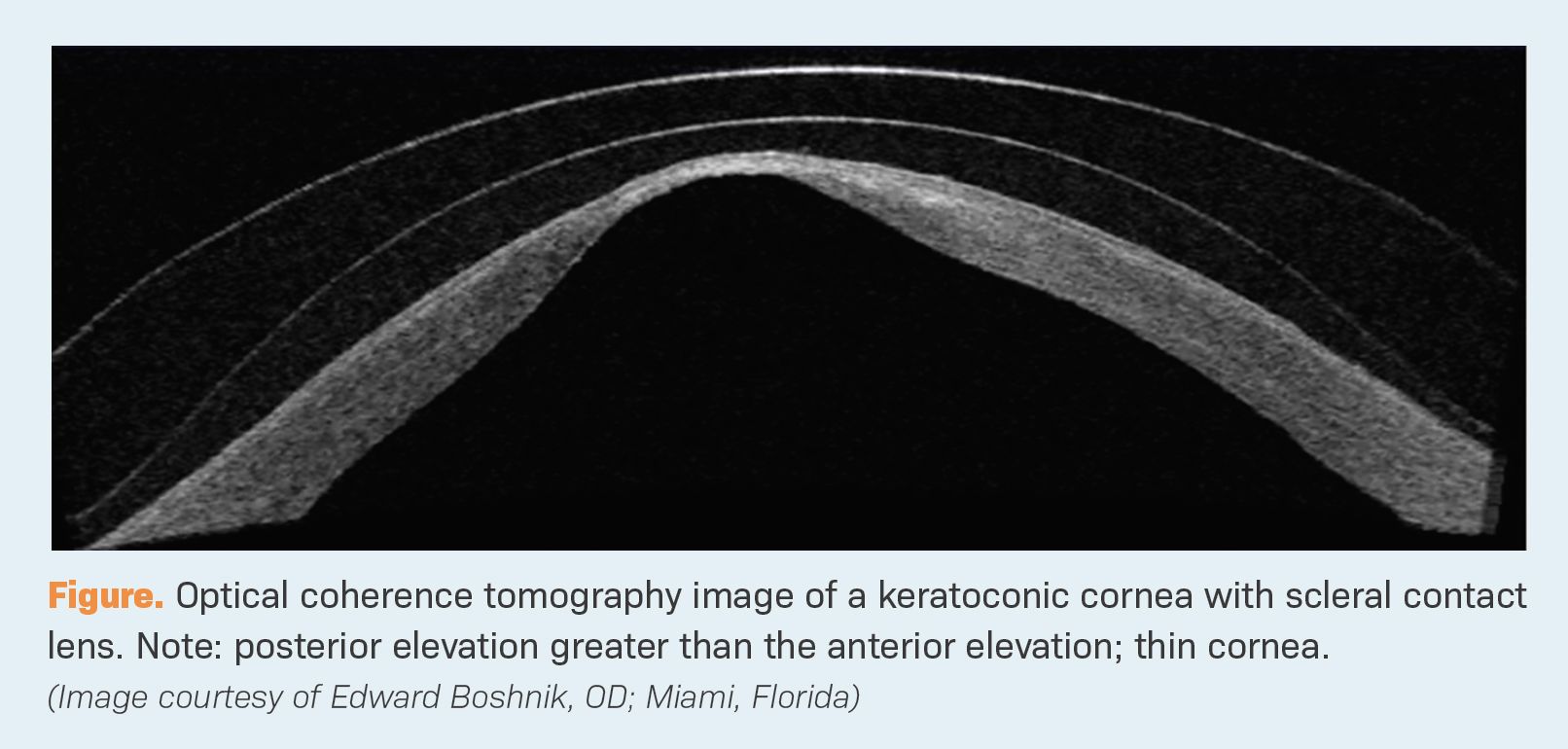
Although most eye care providers diagnose keratoconus with anterior surface curvature topographers, it is important to note that the global consensus group did not use this information as a mandatory finding to diagnose. This is because anterior surface curvature changes are secondary changes from the posterior surface pushing forward. The forces associated with normal or elevated intraocular pressure pushes onto the posterior cornea. In a cornea with collagen of normal thickness and biomechanical strength, the cornea can maintain its normal anatomical shape. In corneas with thin and/or biomechanically weak collagen due to keratoconus, the posterior corneal surface takes on a dynamic movement toward the anterior surface. This action can progressively thin the cornea, elevate the posterior surface, and create a resulting curvature change on the anterior surface. To understand this concept better, think about this: Most keratoconic corneas get steeper and thinner as they get worse. There is no way to get steeper and thinner at the same time unless the posterior surface moves forward at a faster and more significant rate than the anterior surface. This is why particular attention, especially in younger corneas and early phases of the disease, must be paid to the posterior aspect of the cornea.
Definition of ectasia progression
Ectasia progression is defined by a consistent change in at least 2 of the following 3 parameters, where the magnitude of the change is above the normal noise of the testing system: (1) steepening of the anterior corneal surface; (2) steepening of the posterior corneal surface; and (3) thinning and/or an increase in the rate of corneal thickness change from the periphery to the thinnest point.10
General concerns regarding contact lenses for keratoconus
As was well stated in the December 1, 2013, issue of Contact Lens Spectrum by my fellow International Keratoconus Academy of Eye Care Professionals (IKA) board members Barry Eiden, OD, FAAO; Clark Chang, OD, MSA, MSc, FAAO; and colleagues, “contact lenses primarily address the visual challenges of keratoconus by masking the anterior corneal surface irregularity and creating a smoother, more regular anterior optical surface. There are typically 3 key elements to success in all areas of contact lens treatment: (1) providing appropriate vision correction; (2) providing acceptable comfort during lens wear; and (3) providing an appropriate ocular physiological response to lens wear.
Specific to keratoconus, we always want to avoid mechanical pressure on the apex of the cornea, avoid hypoxic stress to the cornea, provide maximum comfort through contact lens fitting design, and optimize vision through contact lens optical design [addressing not only keratoconic visual distortion but also residual astigmatism, presbyopia, and other influences on visual performance].”11
Types of contact lenses for keratoconus:
- Soft spherical and soft toric: If possible, an attempt to improve visual acuity in the keratoconic eye should always be made with soft or soft toric contact lenses. Although visual acuity may be improved with an advanced medical contact lens (hybrid, scleral, EyePrintPRO), comfort and wearing time should be considered as individuals with keratoconus are highly dependent on the vision provided by their contact lens. This increases typical wearing time as opposed to the nonkeratoconic contact lens wearer.
- Rigid gas permeable: These lenses were once the gold standard of keratoconic vision improvement. In some patients, the flat fit of the contact lens would rub against the anterior surface of the cornea, leading to scarring in some cases. Although these are not commonly used in patients with keratoconus anymore, there are still some patients in which this lens is indicated.
- Hybrid/softskirt: Hybrid contact lenses play a role in the continuum of care for keratoconus as they offer the consistent optics of a rigid lens, whereas the periphery provides the comfort and easy adaptation of a soft lens, especially for a patient with newly diagnosed keratoconus. The latest generation available—the UltraHealth lens (SynergEyes)—allows you to maintain the corneal integrity by clearing the apex without overvaulting through reverse geometry curves while also providing maximum oxygen transmission through high-dK materials. For oblate corneas or peripheral ectasias, the UltraHealth FC design allows for flatter base curves with reverse geometry to ensure clearance and tear fluidity.
- Piggyback: This is a combination of soft and hard contact lenses, where the soft contact lens is placed directly on the cornea for initial comfort purposes and a rigid lens is placed on top of the soft lens to improve the quality of vision.
- Scleral: Scleral contact lenses are one of the most successful modalities of contact lenses for keratoconus. The peripheral aspect of the scleral lens rests on the conjunctiva overlying the sclera and episcleral and vaults over the irregular cornea, avoiding contact with the anterior surface of the cornea. In turn, this decreases contact lens–related complications and provides high-quality vision in a large population of those attempting to wear them.
- EyePrint Prosthetics: EyePrintPRO is an optically clear prosthetic impression scleral device designed to match the exact contours of the individual eye, providing the best vision and comfort possible.
In very mild cases of keratoconus, spectacles may provide ample refractive correction. Regardless of the type of contact lens the patient is wearing, it is important to make the patient aware that the contact lens will not slow the progression or worsening of the disease. With any diagnosis of keratoconus, patients must be made aware that rubbing of the eyes has been shown to both worsen the condition and cause it to progress at a faster rate. Additionally, ocular allergy/atopy has also been associated with worsening of disease. Patients with keratoconus and allergy/atopy should be instructed to take antiallergy eye drops.
Corneal CXL
Although contact lenses are a very important component to the continuum of care for patients with keratoconus, if the patient exhibits progression of the disease, CXL treatment may be necessary to intervene and halt progression of the disease. In April 2016, Avedro Inc, a medical device company from Waltham, Massachusetts, was granted FDA approval for their KXL System, Photrexa Viscous (riboflavin 5’-phosphate in 20% dextran ophthalmic solution), and Photrexa (riboflavin 5’-phosphate ophthalmic solution), specifically indicated for progressive keratoconus and postrefractive surgery ectasia.
The treatment, which is currently approved in an epithelial-off technique, is the only FDA commercially available method to halt or slow progression of these visually devastating disorders. Epithelium-off CXL requires the removal of approximately 8 to 9 mm of central corneal epithelium for application and corneal absorption of the Photrexa solution. Once the Photrexa solution has been absorbed throughout the full thickness of the cornea, the KXL UV-A light source can be applied. The reaction between the UV-A light and the riboflavin solution generates a singlet oxygen that is responsible for the CXL.12 After treatment, the eye is irrigated and a bandage contact lens is placed over the open epithelial wound. The cornea is managed postoperatively with ophthalmic antibiotics, steroids, and artificial tears. Short-term postoperative care includes monitoring the cornea for epithelial closure, potential ulcerative keratitis, dry eye, light sensitivity, reticular haze formation, and refractive recovery. Long-term management of the post-CXL cornea includes monitoring for continued progression. The comanaging optometrist must pay particular attention to signs and/or symptoms of progression, including worsening myopia or myopic astigmatic changes, patient complaints of increasing visual blur, corneal thinning, corneal steepening, and posterior or anterior elevation increases on tomography.
If these signs or symptoms of continued progressive keratoconus are identified, a retreatment of CXL may be indicated. Long-term studies show that progression of keratoconus after CXL may occur in approximately 8% of cases.13
Although epithelium-off CXL is the current FDA-approved method of treatment, as of May 1, 2019, Avedro has completed enrollment in a pivotal US phase 3 epithelium-on CXL clinical trial for progressive keratoconus. If this procedure gains FDA approval, this would make treatment and recovery much less painful, with lower rates of infection, inflammation, and corneal haze for the individual receiving treatment. In addition, the visual recovery would be quicker. Currently, there are epithelium-on treatments in the US, but they are not FDA approved.
Through population studies and eye bank information, we know the implementation of CXL as a viable treatment option for progressive keratoconus has reduced the amount of corneal transplants. In Godefrooij et al’s study titled Nationwide Reduction in the Number of Corneal Transplantations for Keratoconus Following the Implementation of Cross Linking, which was extracted from the Dutch National Organ Transplant Registry, approximately 25% fewer corneal transplants were performed in the 3‐year period following the introduction of CXL compared with the 3‐year period prior to the introduction of CXL.14 However, if a corneal transplant does need to be performed for keratoconus, it can either be full or partial thickness in nature. The amount of diseased tissue, overall corneal thickness, and ocular health will dictate the preferred treatment. The posttransplant eye must be monitored frequently for signs of infection, inflammation, ocular disease, refractive error, and transplant rejection.
Management of the pediatric keratoconus cornea
For any clinician, the age of onset of keratoconus is the most important consideration. It has been widely recognized with a near unanimous consensus that younger patients should be examined for change at shorter time intervals, as ectatic change and disease progression can advance rapidly in this group.10 That is to say that if an individual younger than 18 years presents with a primary diagnosis of keratoconus, follow-up visits should be at a maximum of 3-month intervals until either progression stability is absolutely established or a referral for CXL has been made. This clinical reasoning has been based on the paper, Progression of Keratoconus and Efficacy of Pediatric Corneal Collagen Cross-Linking in Children and Adolescents, by Chatzis and Hafezi, which showed that 88% of children diagnosed with keratoconus progressed within 12 months.15
Although this information is very helpful, it did not tell us about the scope of the problem. The IKA felt that this had to be remedied. IKA, in conjunction with the Illinois College of Optometry, undertook a prospective observational study to establish the pediatric prevalence of keratoconus. Knowing these data will provide clinicians evidence on how they need to adjust their clinical practice to properly screen for the disease. In an upcoming edition of this series on keratoconus, we will discuss the incredible results that will change your clinical practice.
Conclusion
Keratoconus is a disease of the cornea that can produce a significant decrease in quality of vision, reduced quality of life, and potentially blindness. We now know that the prevalence and incidence of the disease is much higher than is typically reported in the literature. Keratoconus is not a rare disease. Part of the reason for this is access to new technology that can evaluate the posterior surface of the cornea for early and subtle elevation changes. This information requires optometrists to be on high alert for early evidence of disease. Preservation of best vision will only occur with early detection and proper management. As with all cases of keratoconus, visual improvement with refractive devices, such as standard and advanced medical contact lenses, is critical to patient quality of life.
Optometrists should routinely educate their patients with keratoconus to not rub their eyes and to manage their systemic/ocular allergy and atopy as aggressively as possible, as both have shown to worsen the disease. As increasingly less invasive methods of CXL begin to receive FDA and CE marks of approval, optometrists should be on the forefront of the treatment and management of progressively worsening keratoconic corneas. Early detection is the key to saving vision. The most important consideration in the prevention of keratoconic vision loss is to monitor pediatric keratoconus as early as possible and on a frequent follow-up schedule.
Many thanks for continued discussion, input, and assistance to my fellow IKA board members, Drs Barry Eiden, Clark Chang, Louise Sclafani, Bill Tullo, Loretta Szczotka-Flynn, John Gelles, Steven Sorkin, Chris Sindt, and others. Visit the International Keratoconus Academy website for more information.
References
1. Godefrooij DA, de Wit GA, Uiterwaal CS, Imhof SM, Wisse RP. Age-specific incidence and prevalence of keratoconus: a nationwide registration study. Am J Ophthalmol. 2017;175:169-172. doi:10.1016/j.ajo.2016.12.015
2. Gokul A, Patel DV, McGhee CN. Dr John Nottingham’s 1854 landmark Treatise on Conical Cornea considered in the context of the current knowledge of keratoconus. Cornea. 2016;35(5):673-678. doi:10.1097/ICO.0000000000000801
3. Grzybowski A, McGhee CN. The early history of keratoconus prior to Nottingham’s landmark 1854 treatise on conical cornea: a review. Clin Exp Optom. 2013;96(2):140-145. doi:10.1111/cxo.12035
4. https://www.cdc.gov/csels/dsepd/ss1978/lesson3/section2.html
5. Kennedy RH, Bourne WM, Dyer JA. A 48-year clinical and epidemiologic study of keratoconus. Am J Ophthalmol. 1986;101(3):267–273.
6. Pearson AR, Soneji B, Sarvananthan N, Sanford-Smith JH. Does ethnic origin influence the incidence or severity of keratoconus? Eye (Lond). 2000;14(Pt 4):625-628. doi:10.1038/eye.2000.154
7. Lim N, Vogt U. Characteristics and functional outcomes of 130 patients with keratoconus attending a specialist contact lens clinic. Eye (Lond). 2022;16(1):54-59. doi:10.1038/sj.eye.6700061
8. Cozma I, Atherley C, James NJ, et al. Influence of ethnic origin on the incidence of keratoconus and associated atopic disease in Asian and white patients. Eye. 2005;19(8):924-926. doi:10.1038/sj.eye.6701677
9. Gordon-Shaag A, Millodot M, Shneor E, Liu Y. The genetic and environmental factors for keratoconus. Biomed Res Int. 2015;2015:795738. doi:10.1155/2015/795738

.")




")
Newsletter
Want more insights like this? Subscribe to Optometry Times and get clinical pearls and practice tips delivered straight to your inbox.

















