




















So much basic science research is presented at this meeting, and most of it will be years before it makes its way to clinical trials. Let’s concentrate on research that might be of use to us in the exam room very soon.
Dry Eye
Latest News
Advertisement
CME Content
Advertisement
Scott Schachter, OD, discusses dry eye and how incorporating a dry eye checklist may help improve patient treatment.
Optometry Times Editorial Advisory Board members Leslie E. O’Dell. OD, FAAO, and Scott Hauswirth, OD, FAAO, discuss their recent lecture on inflammation and the role it plays in ocular surface diseases at the American Optometric Association’s Optometry’s Meeting in Washington, DC.
https://www.optometrytimes.com/modern-medicine-cases/new-player-point-care-allergy-testingODs undervalue ocular point-of-care tear testing
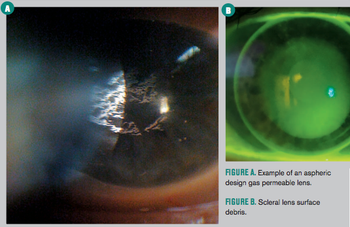
Improve your scleral fitting skills and your patients’ quality of life

The British Contact Lens Association (BCLA) celebrated its 40th birthday June 9-11 at its 2017 clinical conference and exhibition in Liverpool, UK. Optometry Times was there to hear the latest and live tweet from the meeting.
At every age we need adequate, uninterrupted sleep for optimal, wakeful functioning. Insufficient sleep is associated with a number of chronic diseases and conditions such as diabetes, cardiovascular disease, obesity, and depression.
What is this age-defying modern technology that a young, nonmedical professional is applying to her face? It is a YAG laser combined with an intense pulse light (IPL).
David Kading, OD, FAAO, FCLSA, discusses new products, studies, and patient education available to help combat dry eye disease.
Meibomian gland dysfunction (MGD) may be misdiagnosed. While MGD is one of the most common chronic ocular conditions, diagnosing MGD isn’t as simple as it seems.
For the patient, perhaps the most significant symptom of DED is fluctuating or reduced vision.
Mom has pseudoexfoliation syndrome (PXF) clinically visible in both eyes. She experiences pops of elevated intraocular pressure (IOP) in one eye and uses glaucoma medications.
A little over 18 months ago, I decided to follow my passion and take a leap of faith changing my career. I went from a bustling MD/OD group practice to a private group OD practice and launched the Dry Eye Center of Pennsylvania (PA).
Do you reach first for warm compresses or lid scrubs? What about antibiotics? Weigh in!
Prepare your patient by assessing and treating the ocular surface
Recently, much discussion has taken place within the dry eye community regarding the role of punctal plugs in the treatment of dry eye.
SBS signs similar to dry eye
Before the new year gets too far along, let’s take a brief look at the happenings in the pages of Optometry Times during 2016.
The ocular surface encompasses not only the cornea, but the all-important supporting conjunctiva that is divided into the bulbar, limbal, palpebral, forneaceal, and marginal zones.
In the past when you thought of Jennifer Aniston, the girl-next-door character Rachel from Friends would come to mind.
A day in the life of a female patient provides clues that can help
With the exponential increase of interest in dry eye or ocular surface disease (OSD) among physicians and the industry, we are fortunate to have access to exciting new diagnostic and imaging technology as well as new treatment options and therapeutics for some of our most frustrated patients.
There are four reasons to opt for a compounding pharmacy instead of reach for your Rx pad: strength, form, ingredients, and function.
Advertisement
Advertisement
Trending on Optometry Times - Clinical News & Expert Optometrist Insights
1
FDA approves Outlook Therapeutics' Lytenava for wet AMD
2
Detoxifying for visual longevity
3
iVeena completes end-of-phase 1 FDA meeting for IVMED-85 in myopia
4
Orasis Pharmaceuticals, BlinkRx partnership offers new dispensing options for Qlosi
5