



















Glaucoma
Latest News
Advertisement
CME Content
Advertisement
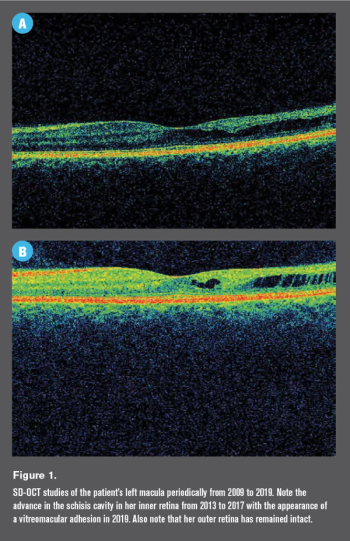
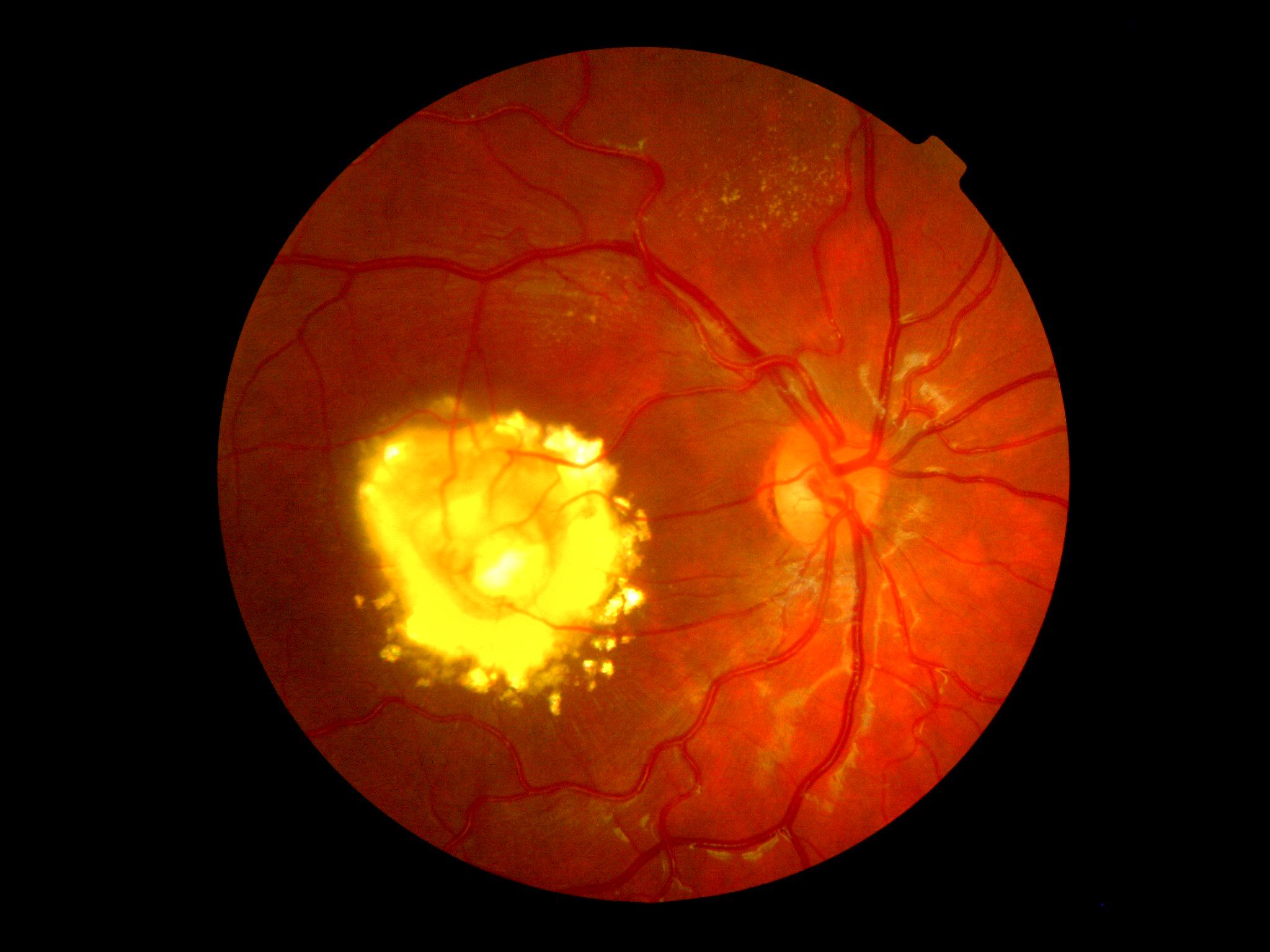
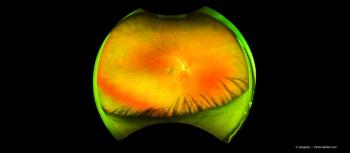
Retinoschisis can make diagnosing open-angle glaucoma especially difficult for optometrists.
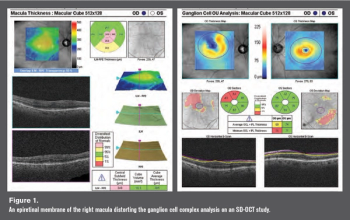
Epiretinal membranes can affect accuracy of a glaucooma diagnosis and disease monitoring

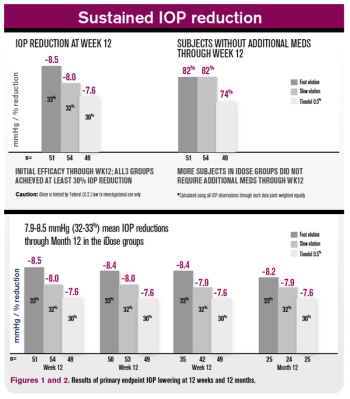
Look beyond intraocular pressure for diagnosis and treatment


Good communication is key when it comes to keeping patient needs at the forefront of care.

A rapid-fire view of 2019’s best innovations in optometry- that stood out the most to ODs.

Misdiagnosing neuropathy and over-reliance on OCT imaging results are two examples










Advertisement
Advertisement
Trending on Optometry Times - Clinical News & Expert Optometrist Insights
1
NIH findings suggest Mediterranean diet associated with slower AMD progression
2
Modern spectacle lenses may halve childhood myopia progression
3
Obesity: New definitions and practical implications to know
4
Encouraging comprehensive eye exams for back to school
5